
 Get Help in Rhode Island
Get Help in Rhode IslandCongenital Diaphragmatic Hernia (CDH)
Guidance for primary care clinicians assessing and managing children with congenital diaphragmatic hernia
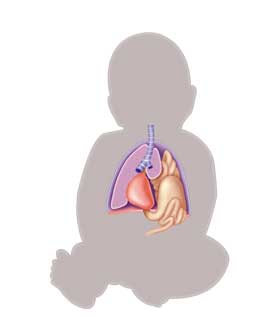
Congenital diaphragmatic hernia (CDH) is an abnormal diaphragmatic development disorder leading to herniation of intra-abdominal content into the thoracic space. This results in underdevelopment of the lungs and pulmonary vasculature with complications of pulmonary hypertension and cardiopulmonary dysfunction.
Key Points
Common long-term problems
Some of the most common long-term
problems in children with CDH are recurrent respiratory system infections (34%),
pathological gastrointestinal reflux (30%), growth delay (20%), and chest wall
deformations/scoliosis (40%). These may occur many years later and often require
consultation with pediatric and/or orthopedic surgery. [Koziarkiewicz: 2014] Children
with CDH also may have respiratory problems, such as chronic lung disease,
aspiration pneumonia, pulmonary hypertension, and obstructive airway disease.
Other common GI issues include oral aversion and growth failure. Neurocognitive
delays and behavioral issues are possible. [Dumpa: 2024]
Surgical morbidities
Herniation recurrence occurs in about
15% of patients with CDH, with the strongest risk factor being a large defect
requiring patch repair. [Jancelewicz: 2013] Patients may be asymptomatic but present
with respiratory distress, hemithoracic bowel sounds, a scaphoid abdomen, and/or
feeding difficulties. The CDH cohort is also at increased risk for small bowel
obstruction.[Jancelewicz: 2013]
[Janssen: 2018]
Important roles of the medical home
The medical home can
assist families with supplemental oxygen, feeding tubes, and other forms of
supportive care and help coordinate follow-up with subspecialists.
Practice Guidelines
Lally KP, Engle W.
Postdischarge follow-up of infants with congenital diaphragmatic hernia.
Pediatrics.
2008;121(3):627-32.
PubMed abstract
Diagnosis
Presentations
Diagnostic Testing & Screening
- Newborn screening
- Hearing screening
- Car seat testing
Imaging
Genetics
Differential Diagnosis
Comorbid Conditions
- Congenital heart disease (all newborns with CDH must undergo echocardiogram)
- Neural tube defects
- CNS malformations
- Genitourinary defects
- Esophageal atresia
- Polysplenia
- Cryptorchidism
- Skeletal abnormalities
- Genetic syndromes
Prognosis
Treatment & Management
Respiratory
Gastro-Intestinal & Bowel Function
Nutrition/Growth
Development
Ears/Hearing
Services & Referrals
- Pediatric Pulmonology (see RI providers [6]) and Pediatric Cardiology (see RI providers [17]) for pulmonary hypoplasia
- Pediatric Gastroenterology (see RI providers [18]) and Dieticians and Nutritionists (see RI providers [3]) if discharging home on tube feedings
- Pediatric Neurology (see RI providers [18]) or Developmental - Behavioral Pediatrics (see RI providers [12]) if necessary
- Pediatric Orthopedics (see RI providers [16]) for scoliosis or chest wall deformities
Support groups for CDH also exist, with a common one being CDH International.
 147 KB)
147 KB)Resources
Information & Support
Related Portal Content
- Autism Spectrum Disorder
- Hearing Screening
- Mental Health Screening for Children & Teens
- Gastroesophageal Reflux Disease
- Developmental Screening
- Feeding Tubes & Gastrostomies in Children
Medical information in one place with fillable templates to help both families and providers. Choose only the pages needed to keep track of the current health care summary, care team, care plan, and health coverage.
Information & Support
For Parents and Patients
Breath of Hope
Detailed information for families in all stages of caring for a child with congenital diaphragmatic hernia. Includes booklets
about expecting a child with CDH, bringing your baby home, how to answer your children's questions about a baby in the NICU,
and managing sensory processing and feeding disorders.
Services for Patients & Families in Rhode Island (RI)
| Service Categories | # of providers* in: | RI | NW | Other states (3) (show) | | NM | NV | UT |
|---|---|---|---|---|---|---|---|---|
| Developmental - Behavioral Pediatrics | 12 | 1 | 2 | 3 | 9 | |||
| Dieticians and Nutritionists | 3 | 1 | 1 | 4 | 6 | |||
| Pediatric Cardiology | 17 | 3 | 4 | 4 | ||||
| Pediatric Gastroenterology | 18 | 2 | 5 | 2 | ||||
| Pediatric Neurology | 18 | 5 | 5 | 8 | ||||
| Pediatric Orthopedics | 16 | 4 | 7 | 8 | 10 | |||
| Pediatric Pulmonology | 6 | 4 | 4 | 3 | ||||
For services not listed above, browse our Services categories or search our database.
* number of provider listings may vary by how states categorize services, whether providers are listed by organization or individual, how services are organized in the state, and other factors; Nationwide (NW) providers are generally limited to web-based services, provider locator services, and organizations that serve children from across the nation.
Helpful Articles
Hollinger LE, Harting MT, Lally KP.
Long-term follow-up of congenital diaphragmatic hernia.
Semin Pediatr Surg.
2017;26(3):178-184.
PubMed abstract
Morini F, Valfrè L, Bagolan P.
Long-term morbidity of congenital diaphragmatic hernia: A plea for standardization.
Semin Pediatr Surg.
2017;26(5):301-310.
PubMed abstract
Page Bibliography
American Academy of Pediatrics Committee on Infectious Diseases; American Academy of Pediatrics Bronchiolitis Guidelines Committee.
Updated guidance for palivizumab prophylaxis among infants and young children at increased risk of hospitalization for respiratory
syncytial virus infection.
Pediatrics.
2014;134(2):e620-38.
PubMed abstract
Arcos-Machancoses JV, Ruiz Hernández C, Martin de Carpi J, Pinillos Pisón S.
A systematic review with meta-analysis of the prevalence of gastroesophageal reflux in congenital diaphragmatic hernia pediatric
survivors.
Dis Esophagus.
2018;31(6).
PubMed abstract
Bojanić K, Pritišanac E, Luetić T, Vuković J, Sprung J, Weingarten TN, Schroeder DR, Grizelj R.
Malformations associated with congenital diaphragmatic hernia: Impact on survival.
J Pediatr Surg.
2015;50(11):1817-22.
PubMed abstract
Chao PH, Chuang JH, Lee SY, Huang HC.
Late-presenting congenital diaphragmatic hernia in childhood.
Acta Paediatr.
2011;100(3):425-8.
PubMed abstract
Danzer E, Hedrick HL.
Neurodevelopmental and neurofunctional outcomes in children with congenital diaphragmatic hernia.
Early Hum Dev.
2011;87(9):625-32.
PubMed abstract
Danzer E, Hoffman C, D'Agostino JA, Gerdes M, Bernbaum J, Antiel RM, Rintoul NE, Herkert LM, Flake AW, Adzick NS, Hedrick
HL.
Neurodevelopmental outcomes at 5years of age in congenital diaphragmatic hernia.
J Pediatr Surg.
2017;52(3):437-443.
PubMed abstract
Dumpa V, Chandrasekharan P.
Congenital Diaphragmatic Hernia.
StatPearls.
2024.
PubMed abstract
Friedman S, Chen C, Chapman JS, Jeruss S, Terrin N, Tighiouart H, Parsons SK, Wilson JM.
Neurodevelopmental outcomes of congenital diaphragmatic hernia survivors followed in a multidisciplinary clinic at ages 1
and 3.
J Pediatr Surg.
2008;43(6):1035-43.
PubMed abstract
Haliburton B, Mouzaki M, Chiang M, Scaini V, Marcon M, Moraes TJ, Chiu PP.
Long-term nutritional morbidity for congenital diaphragmatic hernia survivors: Failure to thrive extends well into childhood
and adolescence.
J Pediatr Surg.
2015;50(5):734-8.
PubMed abstract
Hollinger LE, Harting MT, Lally KP.
Long-term follow-up of congenital diaphragmatic hernia.
Semin Pediatr Surg.
2017;26(3):178-184.
PubMed abstract
Jancelewicz T, Chiang M, Oliveira C, Chiu PP.
Late surgical outcomes among congenital diaphragmatic hernia (CDH) patients: why long-term follow-up with surgeons is recommended.
J Pediatr Surg.
2013;48(5):935-41.
PubMed abstract
Janssen S, Heiwegen K, van Rooij IA, Scharbatke H, Roukema J, de Blaauw I, Botden SM.
Factors related to long-term surgical morbidity in congenital diaphragmatic hernia survivors.
J Pediatr Surg.
2018;53(3):508-512.
PubMed abstract
Koziarkiewicz M, Taczalska A, Piaseczna-Piotrowska A.
Long-term follow-up of children with congenital diaphragmatic hernia--observations from a single institution.
Eur J Pediatr Surg.
2014;24(6):500-7.
PubMed abstract
Lally KP, Engle W.
Postdischarge follow-up of infants with congenital diaphragmatic hernia.
Pediatrics.
2008;121(3):627-32.
PubMed abstract
This guideline was reaffirmed by the American Academy of Pediatrics in 2011.
Leeuwen L, Mous DS, van Rosmalen J, Olieman JF, Andriessen L, Gischler SJ, Joosten KFM, Wijnen RMH, Tibboel D, IJsselstijn
H, Spoel M.
Congenital Diaphragmatic Hernia and Growth to 12 Years.
Pediatrics.
2017;140(2).
PubMed abstract
Longoni M, Pober BR, High FA.
Congenital Diaphragmatic Hernia Overview.
GeneReview.
2020.
PubMed abstract
Maier S, Zahn K, Wessel LM, Schaible T, Brade J, Reinshagen K.
Preventive antireflux surgery in neonates with congenital diaphragmatic hernia: a single-blinded prospective study.
J Pediatr Surg.
2011;46(8):1510-5.
PubMed abstract
McGivern MR, Best KE, Rankin J, Wellesley D, Greenlees R, Addor MC, Arriola L, de Walle H, Barisic I, Beres J, Bianchi F,
Calzolari E, Doray B, Draper ES, Garne E, Gatt M, Haeusler M, Khoshnood B, Klungsoyr K, Latos-Bielenska A, O'Mahony M, Braz
P, McDonnell B, Mullaney C, Nelen V, Queisser-Luft A, Randrianaivo H, Rissmann A, Rounding C, Sipek A, Thompson R, Tucker
D, Wertelecki W, Martos C.
Epidemiology of congenital diaphragmatic hernia in Europe: a register-based study.
Arch Dis Child Fetal Neonatal Ed.
2015;100(2):F137-44.
PubMed abstract
Morandi A, Macchini F, Zanini A, Pasqua N, Farris G, Canazza L, Gentilino V, Di Cesare A, Leva E.
Endoscopic Surveillance for Congenital Diaphragmatic Hernia: Unexpected Prevalence of Silent Esophagitis.
Eur J Pediatr Surg.
2016;26(3):291-5.
PubMed abstract
Morini F, Valfrè L, Bagolan P.
Long-term morbidity of congenital diaphragmatic hernia: A plea for standardization.
Semin Pediatr Surg.
2017;26(5):301-310.
PubMed abstract
Muratore CS, Kharasch V, Lund DP, Sheils C, Friedman S, Brown C, Utter S, Jaksic T, Wilson JM.
Pulmonary morbidity in 100 survivors of congenital diaphragmatic hernia monitored in a multidisciplinary clinic.
J Pediatr Surg.
2001;36(1):133-40.
PubMed abstract
Muratore CS, Utter S, Jaksic T, Lund DP, Wilson JM.
Nutritional morbidity in survivors of congenital diaphragmatic hernia.
J Pediatr Surg.
2001;36(8):1171-6.
PubMed abstract
Peetsold MG, Kneepkens CM, Heij HA, IJsselstijn H, Tibboel D, Gemke RJ.
Congenital diaphragmatic hernia: long-term risk of gastroesophageal reflux disease.
J Pediatr Gastroenterol Nutr.
2010;51(4):448-53.
PubMed abstract
Resch B, Liziczai K, Reiterer F, Freidl T, Haim M, Urlesberger B.
Respiratory syncytial virus associated hospitalizations in children with congenital diaphragmatic hernia.
Pediatr Neonatol.
2018;59(2):184-188.
PubMed abstract
Robertson CM, Cheung PY, Haluschak MM, Elliott CA, Leonard NJ.
High prevalence of sensorineural hearing loss among survivors of neonatal congenital diaphragmatic hernia. Western Canadian
ECMO Follow-up Group.
Am J Otol.
1998;19(6):730-6.
PubMed abstract
Steven MJ, Fyfe AH, Raine PA, Watt I.
Esophageal adenocarcinoma: a long-term complication of congenital diaphragmatic hernia?.
J Pediatr Surg.
2007;42(7):E1-3.
PubMed abstract
Trachsel D, Selvadurai H, Bohn D, Langer JC, Coates AL.
Long-term pulmonary morbidity in survivors of congenital diaphragmatic hernia.
Pediatr Pulmonol.
2005;39(5):433-9.
PubMed abstract